|
|
|
Health Matters Related to Periodontal Diseasebleeding gums contagious diabetes halitosis (breath) heart disease heredity info pages oral cancer cancer treatment periodontal disease pregnancy self test smoking- tobacco women Prevention Treatment Our Office Articles of interest in Periodontics
|
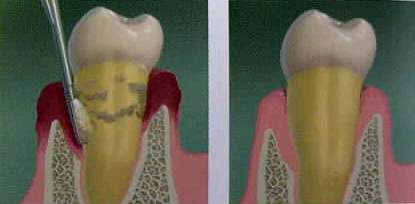
Endoscopically Assisted Root Debridement When I first used The Perioscope during root planing, I had an interesting thought. This was like the difference between trying to see underwater when in a boat and actually scuba diving in The Caribbean. Just as I was spellbound by the coral formations underwater that I had no idea existed, I was equally impressed with the subgingival environment. Suddenly terms like biofilm and tenacious calculus could be associated with visual imagery. The view, as mentioned earlier, was not crystal clear, but it certainly was adequate enough to determine areas that needed additional debridement. Initially, The Perioscope was used as a device to check my work. The full quadrant was root plane with ultrasonics and areas that still felt rough were touched up with Gracy curettes. Then, I would view all of the surfaces with The Perioscope. Residual sites were almost always present. Notable areas included the cementoenamel junctions, furcation entrances and root concavities. In surgery, these are sites where residual calculus is typically found. Finally, the involved surfaces were reinstrumented and efficacy was verified with the scope. In a few cases I would still have to go back for additional debridement. The illustration below depicts one handed imaging of the root and the subsequent endpoint following debridement.
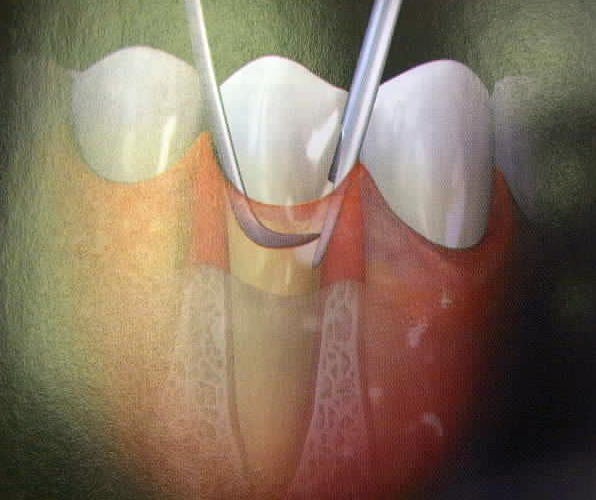
An early lesson I learned was, "just because you can see it, doesn't mean you can remove it." With the scope, one can usually see to 7 mm in most sites. However, the instrumentation was not up to the task without causing undue tissue trauma. At a convention, I found many extended reach instruments of varied designs including curettes, curvettes, hoes and files. With the help of a knowledgeable Dentalview rep, I was able to select several instruments that have made life easier. These instruments enable the clinician to debride many, but not all difficult sites. Unfortunately, surgery still remains the best treatment option for teeth with furcation invasions of grade 2 or more and for teeth with vertical bony defects. Click the image below for an illustration of endoscopy visualization of the furcation region on a lower molar.
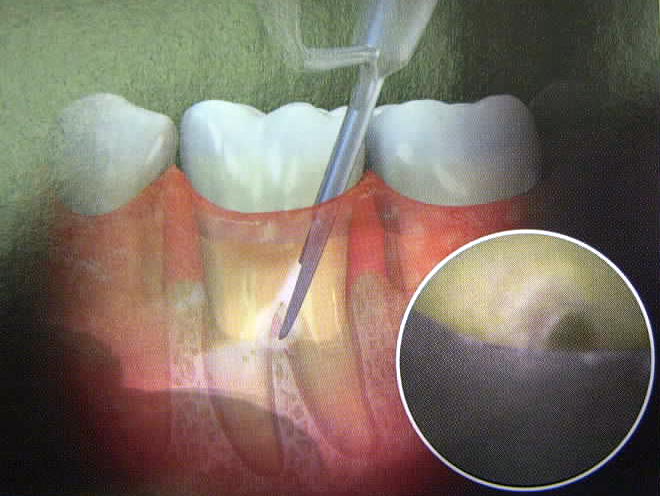
The typical treatment protocol involves scaling and root planing of the entire mouth in the traditional manner. Usually, this is rendered in 1/2 mouth visits. Complete oral hygiene training is given on the first visit, then reviewed in all subsequent appointments. After an appropriate length of time, the patient will be reevaluated. If residual disease is present, a determination will be made as to the best course of action to treat the problem. Everything is weighed at this point to make the proper decision. Root morphology, bone architecture, occlusion, systemic health and behavioral factors are evaluated. If endoscopy is a viable method of treatment, it is presented as an option along with the more traditional approaches such as surgery. Usually, if offered, the patient will choose the non surgical option. For the endoscopy appointment, the patient is prepared in the same manner as our surgical patients. Since these appointments are usually as long as surgical appointments, sedation is offered. They are draped, vitals are taken and then they are administered a local anesthetic. Using the hand typically used to handle a mouth mirror, the operator gently inserts the sheathed endoscope into the periodontal pocket. Vision is established by delicately moving the scope until the proper viewing angle is achieved. The opposite hand uses either an ultrasonic scaler, a curette, or both until the surface is rendered clean. The scope is then moved to the next surface and so on until the area is complete. This two-handed technique is difficult to master, however it dramatically increases the operator's efficiency. Click the photo below for an illustration of root debridement with simultaneous Perioscopic imaging.
The patient is discharged with the same instructions they are typically given following root planing. Oral hygiene resumes the next day. They are asked to return in 2 weeks for plaque removal in the treated area. The treated area will be reevaluated for adequate healing approximately 2 to 3 months following endoscopy. So in summary... The Perioscope has the following indications I. Root Debridement
II. Diagnosis
Dental Endoscopy C.E. Review for Dental Professionals
As always, Aymee and I welcome your referrals and would be happy to discuss any case where you think endoscopy may be beneficial for your patient. Your confidence is appreciated!
Illustrations on this page are courtesy of Dentalview, Inc. Irvine, CA
|